August 18, 2015- by Steven E. Greer, MD
I thought that Tiger Woods, in his prime, was playing the best golf that a human could possibly play. Read more »
May 14, 2015- By Steven E. Greer, MD
Stroke is the bane of TAVR. In the Edwards Lifesciences Sapien valve, stroke rates exceed 10%. That, along with perivalvular leaks, resulted in death rates of 30% at two-years. Read more »
May 31, 2015- By Steven E. Greer, MD
I was watching Green Day give their Rock and Roll Hall of Fame acceptance speech and the singer made some references to smoking pot, as if it was his generation’s thing. I have wondered to myself Read more »
January 14, 2015- Interviewed by Steven E. Greer, MD
We interviewed Dr. Shlomo Melmed, Director of the Clinical Research Institute and Dean of Faculty at Read more »
 Cedars Sinai LA, Diabetes, Endocrinology, FDA, Gastroenterology/Hepatology, Internal medicine, Neurology, OBGYN, Oncology, Pediatrics, Policy, Preventive Medicine | apples49 |
Cedars Sinai LA, Diabetes, Endocrinology, FDA, Gastroenterology/Hepatology, Internal medicine, Neurology, OBGYN, Oncology, Pediatrics, Policy, Preventive Medicine | apples49 |  March 19, 2015 4:24 pm |
March 19, 2015 4:24 pm |  Comments (0)
Comments (0)
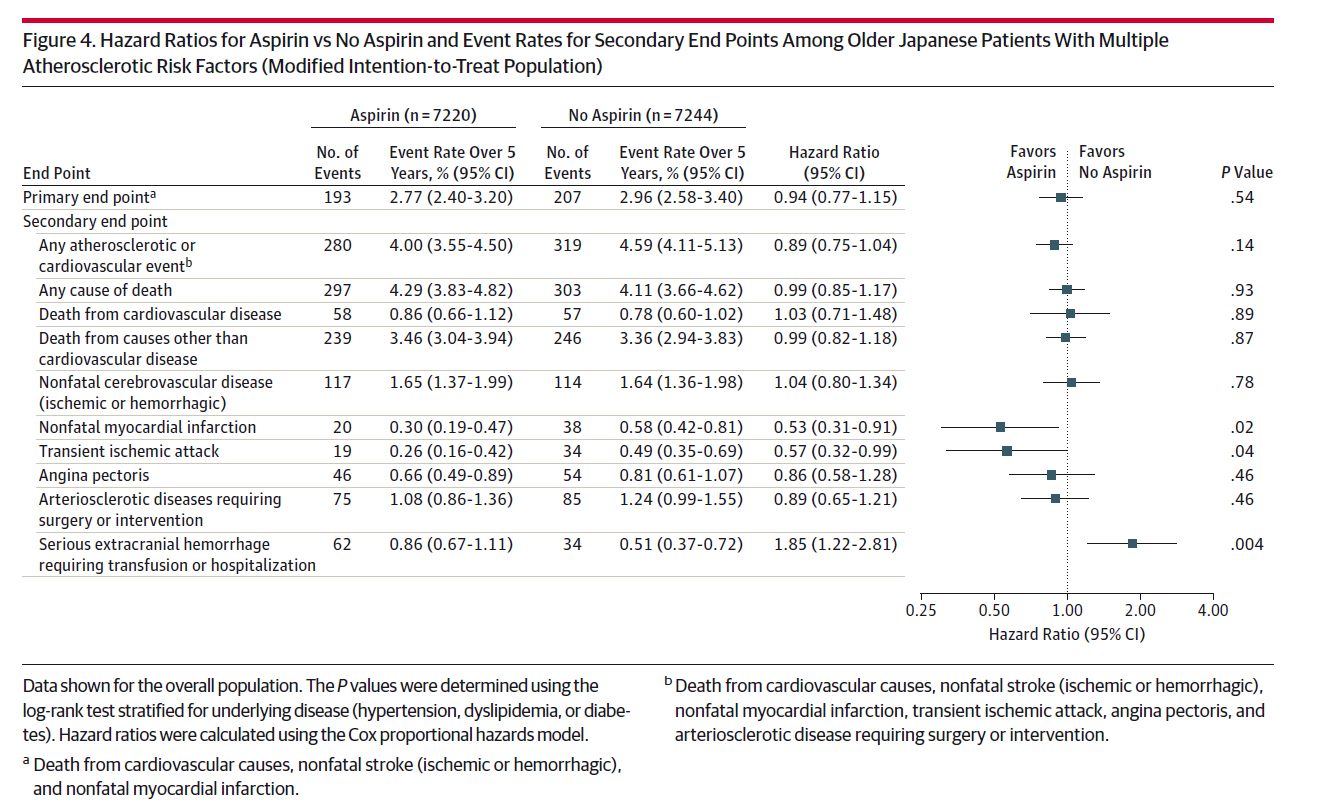
Update January 13, 2015- Yet another study was published highlighting the risks of daily aspirin. Read more »
January 18, 2015- By Steven E. Greer, MD
On July 20th, 2011, the FDA convened an advisory committee to help it determine whether to approve the first ever TAVR device called the Sapien, made by Edwards Lifesciences. I was a public speaker raising the Read more »
Cardiac surgery, Cardiology/interventional, CMS Medicare Medicaid, Columbia University, FDA, JAMA, Medical Devices, Neurology, Op-Ed, Policy, Univ Pennsylvania | apples49 | January 25, 2015 6:58 pm | Comments (0)
 Update January 20, 2015- The PBS news show Frontline has been tracking the number of head injuries in the NFL. The new rules changes that try to eliminate head to head tackling seem to be working. Concussions are Read more »
Update January 20, 2015- The PBS news show Frontline has been tracking the number of head injuries in the NFL. The new rules changes that try to eliminate head to head tackling seem to be working. Concussions are Read more »
Thromboembolic stroke caused by atrial fibrillation is the primary reason patients are placed on anticoagulation. However, those blood thinners also carry significant bleeding risks. As a result, various mechanical surgical approaches have been tried to prevent stroke, and obviate the blood thinners.
The newly approved Boston Scientific Watchman left atrial appendage occlusion device aims to prevent clots from forming and migrating to the brain. We interviewed Dr. William O’Neill of Henry Ford Hospital, a leading interventional cardiologist, about the Watchman, and whether it will truly allow patients with A-fib to stop warfarin or other blood thinners.
December 29, 2010
Many medical devices cause a far greater clinical impact than pharmaceutical therapies such as statins and chemotherapies. For example, ICDs have a dramatic life-saving capability, but for only a small portion of the patients receiving an ICD. Likewise, coronary stents improvement survival in patients with acute MI, but merely alleviate angina in most other patients.
A new device, unknown to most doctors, currently being investigated in Australia, Europe, and South America, could confer the most dramatic clinical benefit to the largest group of patients in the history of medical devices. That device is the Ardian renal artery/nerve ablation catheter to treat essential hypertension, recently acquired by Medtronic.
Medications to treat high blood pressure deliver tens of billions in revenue to the pharmaceutical companies, yet the magnitude of effect is just a few millimeters of mercury reduction in hypertension. In a small, but well designed, trial of the Ardian device, improvements in blood pressure of the magnitude of 30 mmHg were seen in almost all patients. If these data hold up, and safety concerns do not arise, this device would turn the hypertension market upside down, to the dismay of Big Pharma. Total medical costs could be reduced as well if damage to the kidneys, eyes, and hearts of millions of patients are avoided.
Matthews Chacko, MD, Director of Peripheral Vascular Intervention at Johns Hopkins, discusses this device, the data in The Lancet, and his thoughts on safety and efficacy.
Interviewed by Steven Greer, MD
(In full screen 1080 HD for better viewing of the data graphs)
Neurologist S. Claiborne Johnston, M.D., Ph.D. of UCSF reviews the NMT Medical plagued CLOSURE I trial testing the hypothesis that early closure of patent foramen ovales (PFO’s) reduces the incidence of cryptogenic stroke caused by paradoxical emboli. The study was redesigned in midcourse due to slow enrollment. Insurance reimbursement for off-label PFO closure was diverting eligible patients. In addition, some of the patients highest at risk were excluded from the trial.
Dr. Johnston discusses what clinicians should take away from the flawed data and mentions a second similar trial with results expected this year. The larger topic of medical device approval in the U.S. is discussed.